



Part 2: Short acting insulins
Rapid and short acting insulins
After carbohydrate ingestion, insulin is released from the beta in accordance to keep blood glucose in a narrow range. Insulin secretion from the beta cell is thereby under the control of glucose concentrations and modulated by several gastrointestinal signals like intestinal hormones (e.g.GIP or GLP-1) or the autonomic nervous system. Due to insufficient insulin release from the beta cells, numerous patients with diabetes mellitus require exogenous insulin substitution and it is always challenging to tailor exogenous insulin treatment to comply with the physiological requirements. In non-diabetic subjects, after a meal, insulin is released quickly in to the portal blood flow to supress the endogenous glucose release from the liver, and to increase glucose uptake in peripheral tissues. To achieve these physiological needs, subcutaneous insulin application reaches several limitations. The slow absorption of insulin from the subcutaneous tissue often causes pronounced postprandial glucose excursions. In addition, the protracted pharmacodynamic activity can increase the risk of hypoglycaemia in between the meals. Fast acting insulin analogues are gradually replacing conventional mealtime insulins because of their faster absorption and more physiological pharmacodynamic profile (figure 1).
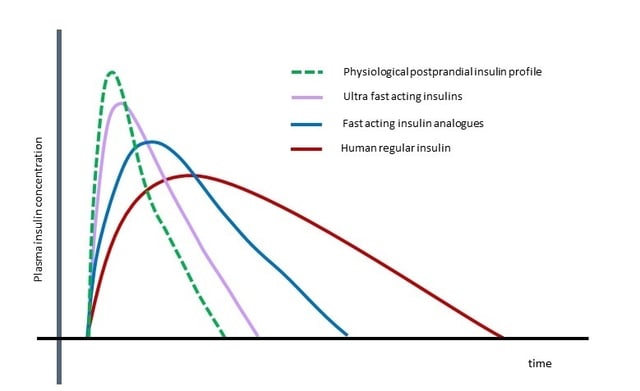
Figure 1: Schematic illustration of the physiological kinetics of postprandial insulin release from the beta cells and the pharmacokinetic properties of different mealtime insulin formulations.
Because of their faster subcutaneous absorption and the better adjustability, fast acting insulin analogues have become the standard insulin for patients using continuous subcutaneous insulin infusion therapy (CSII). Despite the pharmacodynamic advantages of fast acting insulin analogues compared to human regular insulin, they still have certain shortcomings. The peak action of currently available short acting analogues (insulin lispro, insulin aspart , insulin glulisine) occurs about 90 -130 minutes after a subcutaneous injection (1-4), as compared to 30 – 45 minutes taken by endogenous insulin concentrations to peak after a mixed meal intake. New pharmacological and mechanical approaches for mealtime insulin application are under development to better mimic the endogenous insulin profile after a meal.
Addition of excipients
Addition of excipients is one promising approach to speed up the absorption of insulins from the subcutaneous space. Excipients in the insulin formulation can increase the dissociation of insulin molecules, or to modulate the absorption and depression rate of subcutaneous injected insulin formulations. Addition of ethylene diamine tetra acetic acid (EDTA) to human insulin was shown to destabilize the insulin hexamers by chelating the zinc with in the hexameric arrangement of the insulin monomers. In addition, supplementation of citric acid to the formulation masks the surface charge of the insulin monomers, facilitating their vascular penetration (5). Adding these two components to the insulin formulation results in a faster absorption of the insulin from the subcutaneous tissue. In clinical studies, this formulation was shown to provide better postprandial blood glucose control compared to human regular insulin and to the fast acting insulin analogue lispro (6,7). In the formulation of the ultra fast acting analogue insulin aspart (FiAsp), niacinamide is used to fasten the absorption of insulin aspart from the subcutaneous tissue, while arginine is added to enhance the stability of this formulation (figure 2). In glucose clamp studies, FiAsp was shown to have a faster onset and a shorter duration of action compared to the conventional formulation of insulin aspart (8).
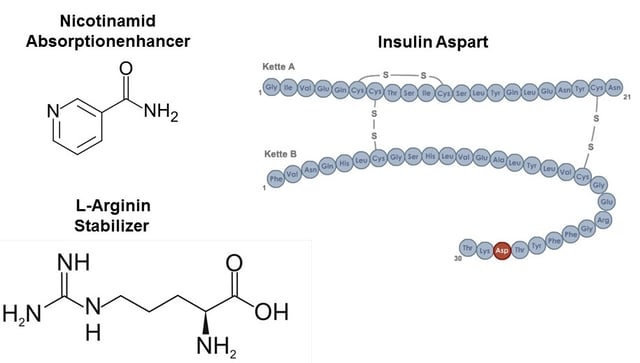
Figure 2: Faster acting insulin analogue aspart (FiAsp) including the excipients nicotinamid to enhance absorption, and L-arginin as a stabilizer
Insulin can be combined with polymers to form reversible molecular complexes which serve for a faster absorption of the insulin molecule from the subcutaneous tissue. Using small oligosaccharide based molecules, insulin lispro was found to provide a faster onset of action with a 60 % reduction of post prandial glucose excursion and less inter subject variability compared to conventional insulin lispro (9,10).
Hyaloronidase is a soluble, neutral pH enzyme that breaks down local hyaluronic acid with in the subcutaneous tissue. Coadministration of Hyaloronidase with regular insulin or fast acting insulin analogues was shown to enhance subcutaneous absorption (11), with a 50% reduced time to achieve peak insulin concentrations and a better control of postprandial hyperglycaemia (12,13).
Insulin delivery
Numerous modifications in the mode of insulin application have been developed to improve the pharmacokinetic properties of insulin. Sprinkler needles used to achieve a vaster subcutaneous spread and to increase the absorption surface failed to significantly affect the pharmacokinetics of subcutaneously applied insulin (14). Jet Injector devices have been developed to provide needle free insulin delivery to the subcutaneous space by the use of high speed and pressure applications (15). Even some studies using this technology provided promising results (16-18), others failed to confirm the improved pharmacokinetic properties using this kind of insulin delivery (19). Intradermal application of insulin by the use of micro needle patches was shown to accelerate the pharmacokinetics compared to subcutaneously injected insulin, covering a shorter time to reach maximal concentration and a lower late insulin exposure (20,21).
Warming of the injection site induces local hyperaemia and accelerates the uptake of insulin from the subcutaneous tissue. A battery powered heating patch (InsuPad®) was shown to accelerate the uptake of human regular insulin and insulin analogues from the subcutaneous tissue with an improvement in postprandial glucose control (22,23). The use of this device in combination with an insulin pump was shown to shorten the time to reach maximum insulin concentration by 35 minutes (24). In obese patients with type 2 diabetes, the use of the heating device was shown to reduce prandial insulin requirements and to lower the rate of hypoglycaemic events (25).
The intrapulmonary route of insulin delivery was investigated in several clinical studies in patients with type 1 and type 2 diabetes mellitus (26). Exubera® was the first pulmonary insulin approved for the use in patients with type 1 and type 2 diabetes mellitus. The pharmacokinetic and pharmacodynamic properties of Exubera® were mostly comparable to the subcutaneous fast acting insulin analogues (27). Exubera® was withdrawn from the market due various reasons including unresolved safety concerns, device handling issues, and a low patient’s acceptance. A second generation pulmonary insulin using human insulin adsorbed onto the excipient fumaryl diketopiperazine microparticles (Afrezza®) was shown with a more rapid onset and shorter duration of action compared with subcutaneously injected rapid insulin analogues (28). Beside these optimized pharmacokinetic and pharmacodynamic properties, this pulmonary insulin formulation possess an enhanced bioavailability and is supplied with an improved inhaler device (Gen2 inhaler®)(29,30). Afrezza® has been approved for the treatment of adults with diabetes mellitus from the US Food and Drug Administration in 2014.
There are several ongoing efforts to develop insulin formulations which can be applied by an oral route. Transmucosal delivery of insulin appears to be suitable, even the bioavailability appears to be low and associated with a high inter- and intra-individual variability. Therefore, several technologies have been developed to improve transmucosal absorption of insulin. Using a buccal delivery system, insulin is applied into the oral cavity by the use of an aerosol application (Oralyn®). The insulin is absorbed through the inside of the cheeks and in the back of the mouth. In clinical studies, buccal insulin was absorbed with a faster onset and a shorter duration of action when compared with subcutaneous insulin (31,32). Application of insulin through the gastro-intestinal route has to overcome several barriers like degradation due to the acid environment in the stomach, a high activity of proteases, and a low absorption rate through the intestine mucosa. Several technologies like coating of insulin, nanocarriers, protease inhibitors, insulin stabilizers, micelles, and microspheres are in development to overcome the challenges of oral insulin application. IN-105 represents a human recombinant insulin molecule conjugated on position B29 with polyethylene glycol via an acetyl chain. In a recent study, IN-105 absorption was found to be proportional to the dose administered. After application of IN-105, the 2-h postprandial glucose excursion was reduced in a dose proportional manner (33). Emisphere oral insulin is based on a noncovalent interaction of the drug-carrier molecule monosodium N-(4-chlorosalicyloyl)-4-aminobutyrate (4-CNAB) with insulin (34). In a glucose clamp study, in male subjects with type 2 diabetes mellitus, Emisphere oral insulin was shown to have a fast onset and a short duration of action, but also was found with a rather high absorption variability in the fasting state (35). Due to the route of insulin absorption into the portal venous system, oral insulins might also provide a hepato-preferential activity of oral insulins.
New insulin pumps in connection with continuous glucose monitors allow for closed loop use of the insulin pump. Recently, the first hybrid closed loop insulin delivery system (MiniMed 670G) was approved for the treatment of diabetes mellitus by the US Food and Drug Administration. To achieve tight glucose control with a closed loop insulin supply systems, the lack time in between the glucose reading and the delivery of insulin to the blood should be brought to a minimum. Therefore, introduction of faster acting insulins is of great interest for the use in those closed loop insulin delivery systems. Faster acting insulin analogues thereby may improve the ability of those closed loop insulin delivery systems. Beside the use of faster absorbed subcutaneous insulins, intraperitoneal application of insulin might be a choice for closed loop insulin delivery systems. In addition to achieve a faster uptake of insulin by peritoneum, the insulin will be drained into the portal circulation providing a hepato-preferential effect of insulin. The use of a port system (AccuCheck Diaport®) for intraperitoneal insulin supply in combination with a closed loop insulin delivery system was shown to lower postprandial glucose excursions with a quicker return to pre meal glucose levels (36).
In conclusion, numerous approaches for ultra rapid insulin delivery are under investigation. Modifications in molecular insulin structure, new insulin formulations or alternate application routes will help to achieve insulin treatments which better mimic the physiological requirements. Most probably this will allow improving glucose control and reducing the risk of hypoglycaemia for patients on insulin treatment, especially for those on a closed loop insulin delivery system.
If this post was interesting to you then check out Part 1 of this series. It deals with the general topic as well as long acting insulins in particular. And make sure to sign up for future blog post updates at the right side of this page.
References :
- Becker RH, Frick AD: Clinical pharmacokinetics and pharmacodynamics of insulin glulisine. Clin Pharmacokinet 47:7-20, 2008
- Nosek L, Roggen K, Heinemann L, Gottschalk C, Kaiser M, Arnolds S, Heise T: Insulin aspart has a shorter duration of action than human insulin over a wide dose-range. Diabetes Obes Metab 15:77-83, 2013
- Lindholm A, Jacobsen LV: Clinical pharmacokinetics and pharmacodynamics of insulin aspart. Clin Pharmacokinet 40:641-659, 2001
- Rave K, Heise T, Weyer C, Herrnberger J, Bender R, Hirschberger S, Heinemann L: Intramuscular versus subcutaneous injection of soluble and lispro insulin: comparison of metabolic effects in healthy subjects. Diabet Med 15:747-751, 1998
- Krasner A, Pohl R, Simms P, Pichotta P, Hauser R, De SE: A review of a family of ultra-rapid-acting insulins: formulation development. J Diabetes Sci Technol 6:786-796, 2012
- Steiner S, Hompesch M, Pohl R, Simms P, Flacke F, Mohr T, Pfutzner A, Heinemann L: A novel insulin formulation with a more rapid onset of action. Int J Obes Relat Metab Disord 51:1602-1606, 2008
- Heinemann L, Hompesch M, Flacke F, Simms P, Pohl R, Albus K, Pfutzner A, Steiner S: Reduction of postprandial glycemic excursions in patients with type 1 diabetes: a novel human insulin formulation versus a rapid-acting insulin analog and regular human insulin. J Diabetes Sci Technol 5:681-686, 2011
- Heise T, Hovelmann U, Brondsted L, Adrian CL, Nosek L, Haahr H: Faster-acting insulin aspart: earlier onset of appearance and greater early pharmacokinetic and pharmacodynamic effects than insulin aspart. Diabetes Obes Metab 17:682-688, 2015
- Andersen G, Meiffren G, Alluis B, Ranson A, Soula R, Gaudier M, Soula O, Kazda C, Heise T, Bruce S: Ultra-Rapid BioChaperone Lispro ameliorates postprandial glucose control compared with Humalog in subjects with type 1 diabetes mellitus. ADA 294-OR: 2016
- Biochaperone insulin (HinsBet). http://www.biocentury.com/products/biochaperone_insulin . 2016.
- Muchmore DB, Vaughn DE: Accelerating and improving the consistency of rapid-acting analog insulin absorption and action for both subcutaneous injection and continuous subcutaneous infusion using recombinant human hyaluronidase. J Diabetes Sci Technol 6:764-772, 2012
- Vaughn DE, Yocum RC, Muchmore DB, Sugarman BJ, Vick AM, Bilinsky IP, Frost GI: Accelerated pharmacokinetics and glucodynamics of prandial insulins injected with recombinant human hyaluronidase. Diabetes Technol Ther 11:345-352, 2009
- Hompesch M, Muchmore DB, Morrow L, Vaughn DE: Accelerated insulin pharmacokinetics and improved postprandial glycemic control in patients with type 1 diabetes after coadministration of prandial insulins with hyaluronidase. Diabetes Care 34:666-668, 2011
- Colagiuri S, Bryson J, Keating S, Tan L, King J, Eigenmann C, Jorgensen KH: Conventional and sprinkler needle injection of magnesium insulin. Diabet Med 9:616-621, 1992
- Romgens AM, Rem-Bronneberg D, Kassies R, Hijlkema M, Bader DL, Oomens CW, van Bruggen MP: Penetration and delivery characteristics of repetitive microjet injection into the skin. J Control Release 234:98-103, 2016
- Hu J, Shi H, Zhao C, Li X, Wang Y, Cheng Q, Goswami R, Zhen Q, Mei M, Song Y, Yang S, Li Q: Lispro administered by the QS-M Needle-Free Jet Injector generates an earlier insulin exposure. Expert Opin Drug Deliv 13:1203-1207, 2016
- de Galan BE, Engwerda EE, Abbink EJ, Tack CJ: Body mass index and the efficacy of needle-free jet injection for the administration of rapid-acting insulin analogs, a post hoc analysis. Diabetes Obes Metab 15:84-86, 2013
- Engwerda EE, Abbink EJ, Tack CJ, de Galan BE: Improved pharmacokinetic and pharmacodynamic profile of rapid-acting insulin using needle-free jet injection technology. Diabetes Care 34:1804-1808, 2011
- Reutens AT, Balkau B, Cohen N: A pilot study to examine the tolerability and device preference in type 1 diabetes of insulin aspart administered by InsuJet compared with subcutaneous injection. Diabetes Technol Ther 16:235-240, 2014
- Hultstrom M, Roxhed N, Nordquist L: Intradermal insulin delivery: a promising future for diabetes management. J Diabetes Sci Technol 8:453-457, 2014
- Kochba E, Levin Y, Raz I, Cahn A: Improved Insulin Pharmacokinetics Using a Novel Microneedle Device for Intradermal Delivery in Patients with Type 2 Diabetes. Diabetes Technol Ther 18:525-531, 2016
- Raz I, Bitton G, Feldman D, Alon T, Pfutzner A, Tamborlane WV: Improved Postprandial Glucose Control Using the InsuPad Device in Insulin-Treated Type 2 Diabetes: Injection Site Warming to Improve Glycemic Control. J Diabetes Sci Technol 9:639-643, 2015
- Freckmann G, Pleus S, Haug C, Bitton G, Nagar R: Increasing local blood flow by warming the application site: beneficial effects on postprandial glycemic excursions. J Diabetes Sci Technol 6:780-785, 2012
- Raz I, Weiss R, Yegorchikov Y, Bitton G, Nagar R, Pesach B: Effect of a local heating device on insulin and glucose pharmacokinetic profiles in an open-label, randomized, two-period, one-way crossover study in patients with type 1 diabetes using continuous subcutaneous insulin nfusion. Clin Ther 31:980-987, 2009
- Pfutzner A, Raz I, Bitton G, Klonoff D, Nagar R, Hermanns N, Haak T: Improved insulin absorption by means of standardized injection site modulation results in a safer and more efficient prandial insulin treatment. A review of the existing clinical data. J Diabetes Sci Technol 9:116-122, 2015
- Diez JJ, Iglesias P: Inhaled insulin--a new therapeutic option in the treatment of diabetes mellitus. Expert Opin Pharmacother 4:191-200, 2003
- Rave KM, Nosek L, de la Pena A, Seger M, Ernest CS, Heinemann L, Batycky RP, Muchmore DB: Dose response of inhaled dry-powder insulin and dose equivalence to subcutaneous insulin lispro. Diabetes Care 28:2400-2405, 2005
- Kim ES, Plosker GL: AFREZZA(R) (insulin human) Inhalation Powder: A Review in Diabetes Mellitus. Drugs 75:1679-1686, 2015
- Boss AH, Petrucci R, Lorber D: Coverage of prandial insulin requirements by means of an ultra-rapid-acting inhaled insulin. J Diabetes Sci Technol 6:773-779, 2012
- Heinemann L, Baughman R, Boss A, Hompesch M: Pharmacokinetic and Pharmacodynamic Properties of a Novel Inhaled Insulin. J Diabetes Sci Technol 2016
- Heinemann L, Jacques Y: Oral insulin and buccal insulin: a critical reappraisal. J Diabetes Sci Technol 3:568-584, 2009
- Cernea S, Kidron M, Wohlgelernter J, Modi P, Raz I: Dose-response relationship of oral insulin spray in healthy subjects. Diabetes Care 28:1353-1357, 2005
- Khedkar A, Iyer H, Anand A, Verma M, Krishnamurthy S, Savale S, Atignal A: A dose range finding study of novel oral insulin (IN-105) under fed conditions in type 2 diabetes mellitus subjects. Diabetes Obes Metab 12:659-664, 2010
- Malkov D, Angelo R, Wang HZ, Flanders E, Tang H, Gomez-Orellana I: Oral delivery of insulin with the eligen technology: mechanistic studies. Curr Drug Deliv 2:191-197, 2005
- Kapitza C, Zijlstra E, Heinemann L, Castelli MC, Riley G, Heise T: Oral insulin: a comparison with subcutaneous regular human insulin in patients with type 2 diabetes. Diabetes Care 33:1288-1290, 2010
- Renard, E. M. Artificial pancreas: is it safe and efficient in daily life? EASD Munich OP #28.1. 2016.